Radical Prostatectomy Surgery
Radical prostatectomy implies the complete removal of the prostate gland along with the pelvic lymph nodes.
Radical prostatectomy surgery may be performed by either a retropubic or perineal approach. Most surgeons prefer the retropubic approach, as it allows access to the pelvic lymph nodes and the simultaneous performance of a lymph node dissection. In addition, contemporary surgery techniques for urethral anastomosis have very low complication rates with good continence, and wider excision or preservation of the neurovascular bundles may be more easily affected. Although perineal prostatectomy surgery has the potential advantages of lower blood loss and more direct urethral anastomosis, these advantages may be outweighed by the lack of periprostatic fascias that are removed together with the prostate. During perineal prostatectomy, the dissection is performed essentially along the prostatic gland, whereas the primary dissection during retropubic prostatectomy is performed outside of the prostatic fascias.
Since the radical prostatectomy introduction by Millen in 1947, the retropubic approach to prostatectomy has been a standard treatment. However, the popularity of this procedure was poor until the last 20 years because of the frequent complications of bleeding, incontinence, and impotence. More recently, anatomic discoveries have improved surgeons' ability to remove all of the tumor and substantially decrease associated morbidity. Delineation of the periprostatic vascular anatomy, the relationship of the neurovascular bundles to the prostate, and subsequent evaluation of the periprostatic urethral sphincter mechanism have decreased perioperative blood loss. In addition, improved postoperative potency and urinary continence rates have been achieved. Many of these advances are based on the anatomic work described by Walsh and others at the James Buchanan Brady Urological Institute of the Johns-Hopkins Hospital (Reiner & Walsh, 1979; Walsh et al., 1983; Walsh, 1987).
One primary source of potential bleeding during prostatectomy is the dorsal vein complex that passes over the prostate gland. The dorsal vein complex enters the pelvis under the pubic bone. It is located just above the urethral sphincter muscles and below the periprostatic fascias. The dorsal vein complex is opened during the division of the fascia and urethral sphincter. Control of this vascular structure is usually performed with sutures. It must be performed carefully to avoid compromising urethral sphincter function. The dorsal vein complex from the penis then fans out over the prostate, and it must be further secured on the lateral and superior portions of the prostate during completion of the prostatectomy (Reiner & Walsh, 1979).
The autonomic innervation of the penis travels in the cavernous nerves that are located just posterolateral to the prostate in close association with the lateral prostatic fascia and rectum. These nerves are derived from branches of the pelvic plexus that lie in a fenestrated plate along the lateral sidewall of the rectum between 5 and 11 cm from the anal verge. The pelvic plexus is derived from hypogastric nerves that travel laterally to the sigmoid colon and sacral roots 2, 3, and 4, which provide parasympathetic efferent preganglionic fibers. For patients in whom it is clinically appropriate to preserve the cavernous nerves, their location can be identified because they travel with the capsular veins of the prostate in a group posterolateral to the prostate. This neurovascular bundle complex is outside the prostate (Schlegel & Walsh, 1987). Preservation of the neurovascular bundle does not result in any compromise to the removal of the entire prostate with its capsule.
The neurovascular bundle can be isolated and preserved during radical prostatectomy by incising the lateral prostatic fascia just anterior to the neurovascular bundle. After small branches of the neurovascular bundle to the prostate are clipped and divided, the neurovascular bundle stays on the rectal surface in close association with the lateral prostatic fascia as the prostate is removed. The striated urethral sphincter surrounds the urethra and attaches to the prostate. Preservation of this urethral sphincter complex is critical to the early and effective restoration of continence for men after radical prostatectomy. Again, the striated urethral sphincter is outside of the prostate. Division of the striated urethral sphincter may be carried out under direct vision during apical dissection of the prostate. Direct incision of this region may be effected after dorsal vein complex control is obtained. Maintenance of an optimal urethral sphincter (striated) muscle length is important. During all portions of the apical dissection, the surgeon must be confident that the entire prostate is removed and only the urethral muscle is preserved. Re-establishment of the striated urethral sphincter muscle relationship to the puboprostatic ligaments and periurethral fascias around the dorsal vein complex is essential to provide a normal anatomic relationship between the urethra and the pubis postoperatively.
Preoperative Preparation
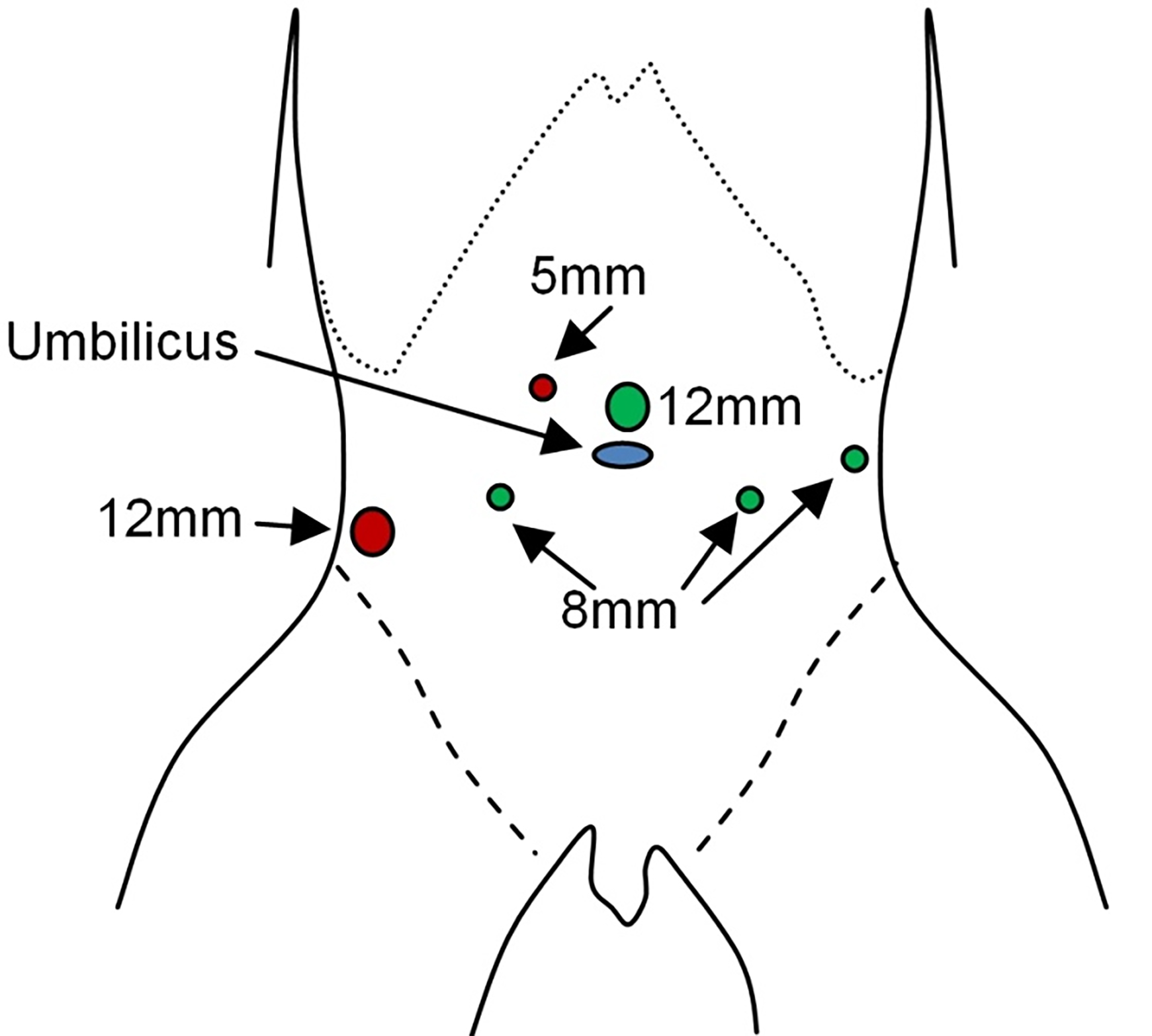
Surgery is often deferred for six to eight weeks after needle biopsy of a prostate and 12 weeks after transrectal resection to allow resolution of any inflammatory reaction that may occur from these biopsies. With the newer 18-gauge needle biopsies of the prostate, periurethral and periprostatic inflammation is typically minor. Some patients will choose to have autologous blood stored preoperatively or to receive recombinant erythropoietin preoperatively to decrease their risk of receiving heterologous blood transfusion. Patients may receive a limited bowel preparation with magnesium citrate and should have an enema the morning before surgery. Many surgeons prefer a regional or a spinal anesthetic for this operation. Regional anesthesia is associated with lower blood loss and a decreased risk of deep venous thrombosis and pulmonary emboli. Since pulmonary emboli are the most common cause of perioperative mortality, the use of epidural anesthesia is supported (Peters and Walsh, 1985; Malhotra et al., 1996). The patient is placed supine on the table, which is flexed to extend the distance between the umbilicus and the pubis. The position of table flexion is initially located at the level of the umbilicus. The patient is prepped and draped with the phallus, available for manipulation during the procedure. A 16- to 18-French Foley catheter is placed per urethra with 40 to 50 cc in the Foley catheter balloon. A standard lower abdominal midline incision is fashioned, and the retroperitoneal space is opened. Direct care should be taken to open the transversalis fascia sharply, as preservation of this structure may be essential to prevent postoperative hernia formation. The peritoneum is then mobilized superiorly on both sides up to the iliac vessels and psoas muscle level if lymph node dissection is planned.
Surgical procedure
Sampling lymph node dissection is performed in the obturator space, with the lateral margin of dissection being the pelvic wall and external iliac vein, the distal margin being the node of Cloquet, and the proximal margin being the hypogastric vessels. The posterior margin is the obturator nerve within the pelvis. Removal of the obturator vessels is neither helpful nor beneficial. Occasionally, the obturator artery provides blood supply to the phallus, and removing the obturator artery may compromise penile blood flow. A self-retaining retractor, such as the Balfour retractor, is used during the procedure. A retracting arm with a notched blade, such as the Yu-Holtgrewe blade, can retract the Foley catheter superiorly within the bladder. This provides optimal access to the prostate and its attachments to the pubis.
The endopelvic fascia is then defined by removing any fat from this structure, and an incision is fashioned sharply in the endopelvic fascia just lateral to the capsular veins of the prostate. Care should be taken during this time to incise only the fascia. This incision allows separation of the endopelvic muscles from the prostate. Small veins in this region may be controlled with electrocautery. After incision in the endopelvic fascia on both sides, the prostate can now be moved laterally to allow better access to the apex. At this point, a running suture of 0 or 20 chromic can be placed into the fascia, overlying the prostate from the midportion of the prostate and laterally on each side over its anterior surface. This allows the dorsal vein vessels to be trapped between the fascia and the prostate. This maneuver decreases back bleeding through the dorsal venous complex over the prostate. The fascia covering the prostate is then divided sharply, including the puboprostatic ligaments' division. Separation of the puboprostatic ligaments from the pubic symphysis is discouraged, as this prevents the re-establishment of the normal urethral sphincter relationship to the pubic bone through its reattachment to the periurethral fascias. The dorsal vein complex is then entered and oversewn with 2-0 or 3-0 absorbable sutures. As noted above, care must be taken to avoid extending these sutures into the urethral sphincter complex, which may limit its postoperative function. The striated urethral sphincter and anterior urethra are then divided just distal to the apex of the prostate. Removal of an excess length of urethral sphincter muscle does not improve cancer control and can increase the risk of postoperative incontinence.
Care should be taken to divide the urethral muscle around the Foley catheter. The posterior portion of the urethra is not directly visualized at this point and is not divided. The urethral sphincter sutures can then be placed for the subsequent urethro-vesicle anastomosis. Viewed from the patient's head, sutures are placed at 6 o'clock, 8 o'clock, 10 o'clock, 12 o'clock, 2 o'clock, and 4 o'clock. Placement of the sutures at this time is easy to affect by pushing the prostate inferiorly, and sutures are placed in an inside-out fashion only for the 12 o'clock suture. Other sutures are placed in an outside-in fashion. For the anterior sutures, the urethral mucosa and a small cross-segment of urethral muscle are included, as well as the anterior segment of fascia that was previously above the urethral sphincter. This allows restoration of the normal urethral angle postoperatively. After five of these six sutures have been placed, the catheter is brought up through the incision in the urethra and retracted cephalad. The 6 o'clock suture can then be placed in the posterior urethra. A right-angle clamp is placed behind the urethra, and the posterior segment of the urethra is divided sharply. Attention may then be turned to the lateral prostatic fascias.
The prostate is rolled laterally without excessive traction on the urethral catheter. The lateral prostatic fascia alone is divided just above the neurovascular bundle complex at the posterolateral level of the prostate. Small vessels that come off of the neurovascular bundle are identified and clipped. The prostate should then be released from the neurovascular bundle at the apical level.

The Denonvilliers' fascia can then be easily identified, and a right-angle clamp is placed behind Denonvilliers' fascia and the posterior portion of the urethral sphincter muscle at the level of the apical prostate. Care must be taken at this point to avoid an incision into the posterior portion of the prostate. Blunt dissection on the rectum at this point should be avoided to prevent tearing or neuropraxia to the neurovascular bundles. While neurovascular bundles are still attached to the prostate, they are highly susceptible to traction injury. The Denonvilliers' fascia is then incised just medial to the neurovascular bundle, freeing the bundle from the prostate.
In cases where it is appropriate to unilaterally or bilaterally perform wide excision of the neurovascular bundle, the neurovascular bundle is isolated at the level at the apex of the prostate, and absorbable sutures are used to tie this neurovascular bundle complex. A right angle should be placed entirely around the neurovascular bundle, and care should be taken to avoid entry into the rectum at this point. An incision in the lateral prostatic fascia for wide excision of the neurovascular bundle is performed posterior to the bundle itself.
After the urethral sphincter is divided posteriorly by Denonvilliers' fascia, the prostate may then be mobilized up to the level of the posterolateral base of the prostate near its junction with the bladder. Major vessels and branches of the inferior vesicle artery entering the prostate should be secured at this level with clips or ligatures. After the prostate is mobilized laterally, Denonvilliers' fascia is then incised over the level of the seminal vesicles. This allows dissection along the seminal vesicles up laterally over the bladder. An arterial complex is typically found anterior to the seminal vesicle on each side, between the seminal vesicle and the bladder. This arterial complex should be specifically ligated before its division. Attention may then be turned to the anterior surface of the bladder and prostate junction. The bladder is entered with care taken to avoid entry into the prostate. The best maneuver to prevent entry into the prostate is to maintain dissection on the bladder muscle itself. Once the bladder has been widely opened, the Foley catheter balloon may be deflated, and both ends of the Foley catheter may be used to retract the prostate inferiorly.
After intravenous infusion of indigo carmine, blue efflux from the ureteral orifices may be directly identified. This can be used to avoid incision into the ureteral orifices. The bladder muscle may then be divided posteriorly, leaving the prostate specimen attached only by its seminal vesicles and vas deferens. Midline dissection is then performed to isolate the vas deferens that are separated from the seminal vesicle along its entire length. Separation of the vas from the seminal vesicle allows identification of the vessels at the superior margin of the seminal vesicles. The vas deferens and its associated vessels are clipped and divided. Attention is then turned to the seminal vesicles that are dissected down to their vessels located at the superior portion of the seminal vesicles. Care must be taken to avoid avulsion of these vessels or the seminal vesicle.
The seminal vesicle blood supply is clipped and divided, and the prostate specimen can be removed. An initial review for bleeding within the pelvis should be performed. The bladder neck can then be narrowed in a tennis-racquet fashion. Initial sutures of 2-0 chromic are placed at the level of the ureteral orifices to re-approximate the bladder muscle. The bladder is closed along its length. An approximately 30-French opening is left at the anterior portion of the bladder neck closure. The urethral mucosa can be everted with 4-0 sutures to improve the opportunity for mucosa-to-mucosa anastomotic connection postoperatively. The sutures previously placed into the urethra can then be placed correspondingly at 12-, 2-, 4-, 6-, and 10 o'clock. These sutures are placed after a new urethral catheter has been placed and brought up anteriorly within the pelvis. The Foley catheter is placed into the bladder before placement of the 12 o'clock suture but after placement of all other sutures.
The urethro-vesical anastomosis is then completed by tying the sutures circumferentially around the urethro-vesical anastomosis. I prefer to use 2-0 or 3-0 Monocryl sutures for the anastomosis, as they tie easily, are fairly rapidly absorbed after healing of the anastomosis, and are durable sutures. The anastomosis has no gaps, and the bladder should come down quickly. Suppose there is difficulty in bringing the bladder down to the urethra. In that case, the obliterated umbilical artery should be divided, the flexion should be decreased on the operating table, and the peritoneal reflection should be freed up laterally to allow the bladder to more easily reach the urethra without tension.
Pelvic drains may then be placed into the lower abdomen to collect any urethral leakage that may occur from the anastomosis preoperatively, as well as lymphatic fluid. If clinically detectable hernias are present, they may be repaired at this time. Simultaneous preperitoneal repair of hernias in men undergoing radical prostatectomy may be effectively accomplished with polypropylene mesh, with low morbidity and excellent results (Choi et al., 1999).
Perineal prostatectomy
The perineal approach is performed with the patient in the exaggerated lithotomy position. The perineum is opened, and dissection is performed around the external rectal sphincter fibers. The rectourethralis muscle is divided, and Denonvilliers' fascia is left on the prostate. The vascular pedicles to the prostate are ligated at the prostate base, the seminal vesicles and vasa deferentia are isolated and removed, and the prostate is separated from the bladder. Anastomosis is carried out to the urethral stump after removal of the prostate.
Results after prostatectomy
Patients after radical prostatectomy should have an undetectable PSA level. Systemic PSA detection (>0.2 ng/mL) indicates recurrent local or systemic disease. The risk of biochemical recurrence depends on the tumor's local extent (organ-confined vs. extracapsular penetration), invasion of seminal vesicles or lymph nodes, and Gleason sum score. Long-term overall results from Johns Hopkins Hospital are presented in Figure . However, Gleason score and extent of local disease in the prostatic specimen provides a far more accurate means of estimating the risk of disease recurrence (Pound et al. 1997).
Results for return of urinary control after prostatectomy vary greatly from surgeon to surgeon in different series, urinary control returns for 75-98% of patients postoperatively. Return of erectile function may take up to 12-18 months, and achievement of erections adequate for vaginal penetration and climax occur in 40-80% of men in selected series, based on the number of neurovascular bundles preserved, age of the patient, preoperative erectile function, and extent of tumor.